机构名称:
¥ 1.0
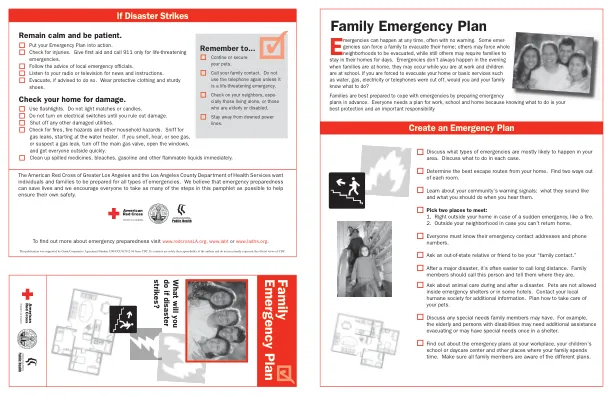
Family Information Name: ___________________________________ Phone: _______________ Date of Birth: __________ Medical Information/Allergies: ___________________________________________________________ Name: ___________________________________ Phone: _______________ Date of Birth: __________ Medical Information/Allergies: ___________________________________________________________ Name: ___________________________________ Phone: _______________ Date of Birth: __________ Medical Information/Allergies: ___________________________________________________ Name: ___________________________________ Phone: _______________ Date of Birth: __________ Medical Information/Allergies: ___________________________________________________________ Name: ___________________________________ Phone: _______________ Date of Birth: __________ Medical Information/Allergies: ___________________________________________________________
家庭紧急准备计划
主要关键词
相关文件推荐