机构名称:
¥ 1.0
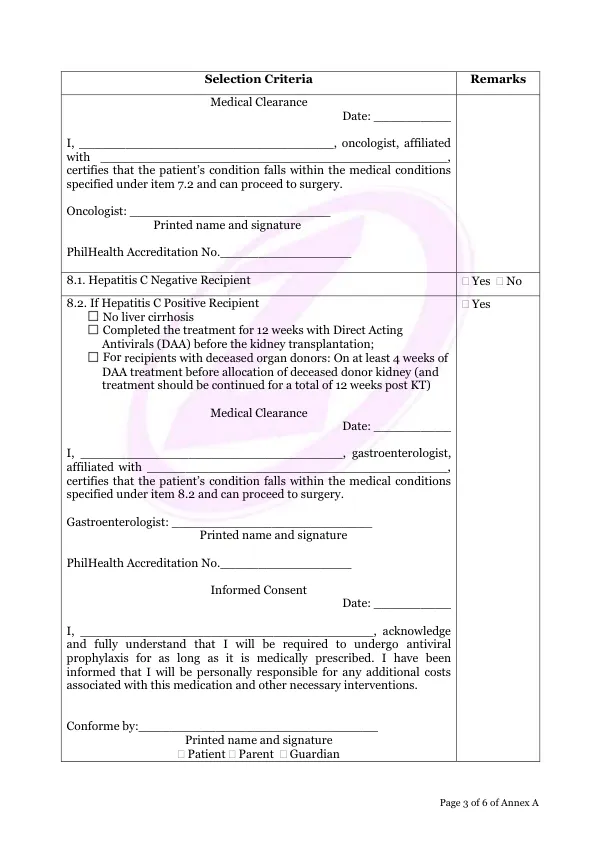
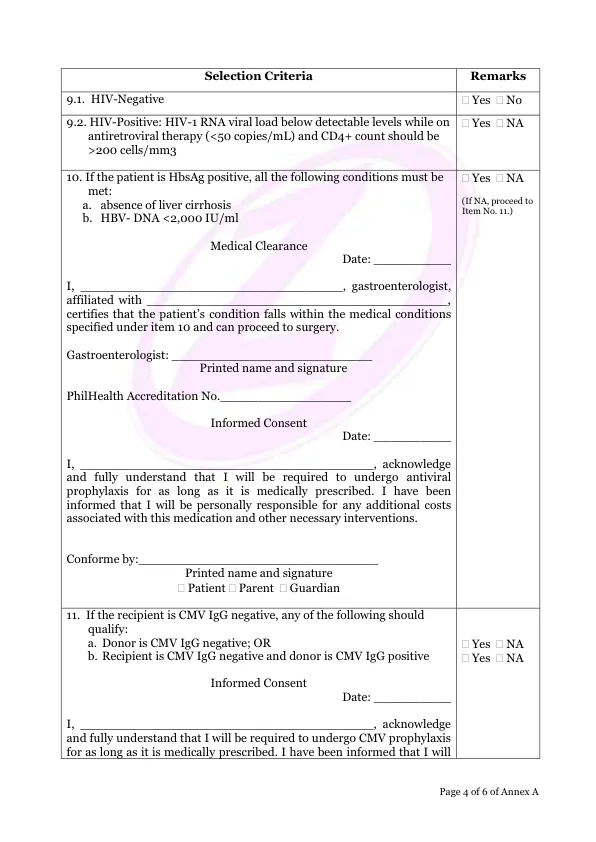
Date: __________ I, ______________________________________, acknowledge and fully understand that I will be required to undergo antiviral prophylaxis for as long as it is medically prescribed.我被告知,我将对与这种药物相关的任何额外费用和其他必要的干预措施负责。符合:__________________________________
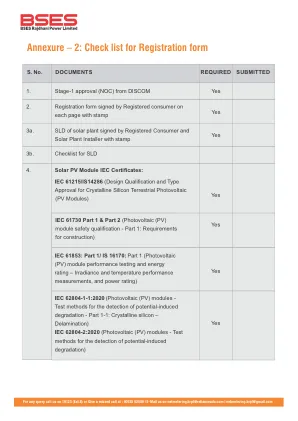
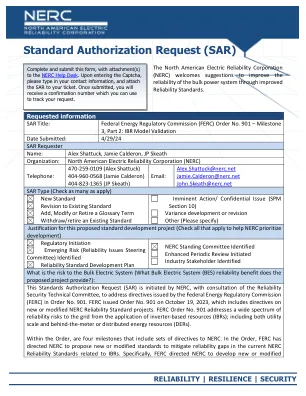
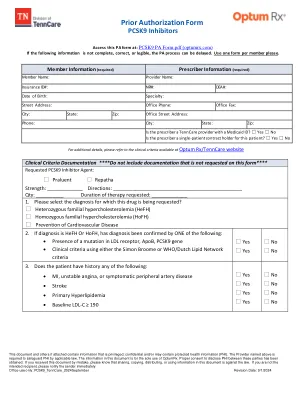
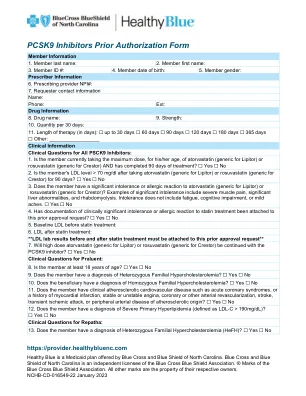
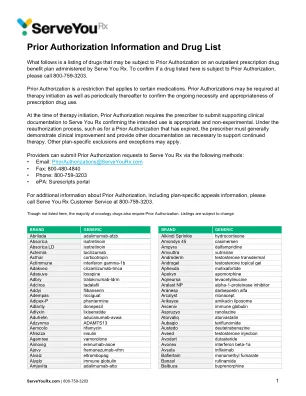
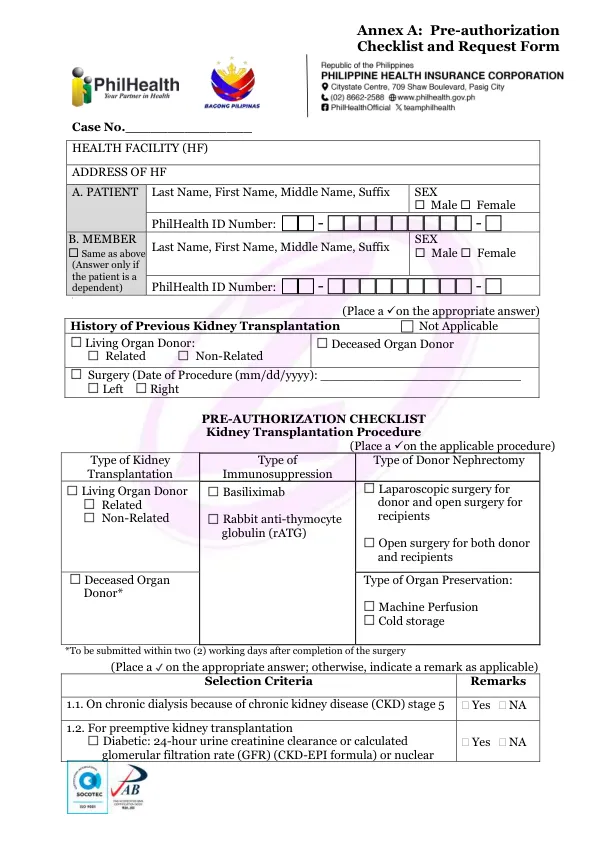
附件A:预授权清单和请求表格
主要关键词

相关文件推荐