机构名称:
¥ 1.0
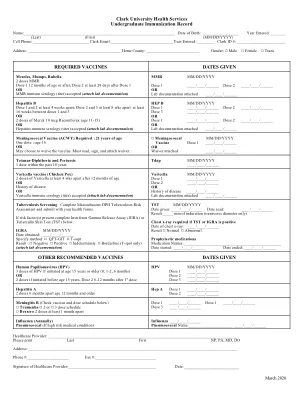
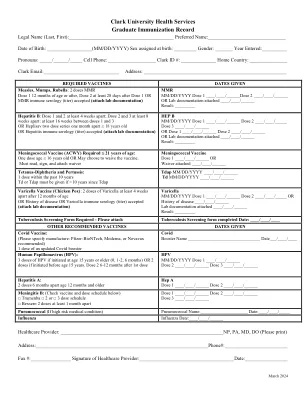
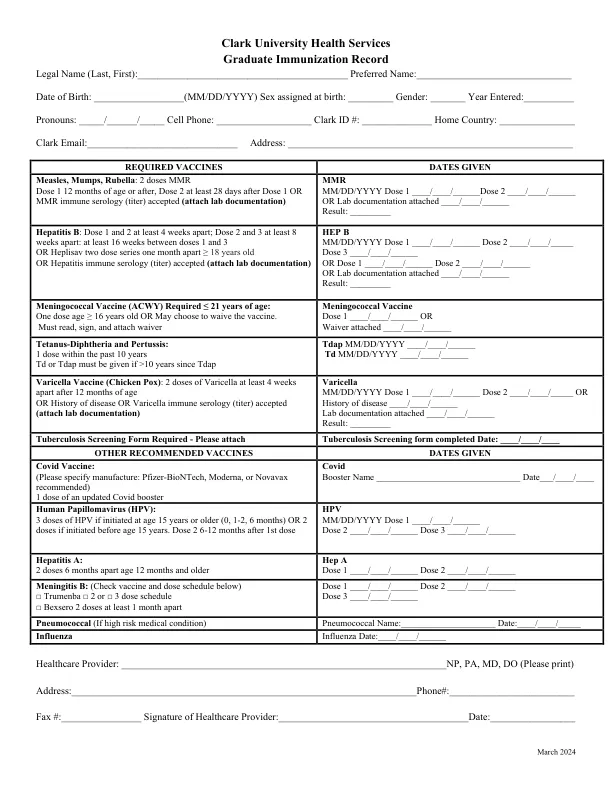
Graduate Immunization Record Legal Name (Last, First):__________________________________________ Preferred Name:_______________________________ Date of Birth: __________________(MM/DD/YYYY) Sex assigned at birth: _________ Gender: _______ Year Entered:__________ Pronouns: _____/______/_____ Cell Phone: ___________________ Clark ID #: ______________ Home Country: _______________ Clark Email:______________________________ Address: _________________________________________________________
毕业生免疫记录
主要关键词
相关文件推荐