XiaoMi-AI文件搜索系统
World File Search Systemsymptom
有关更新的国家癌症战略的建议
6.5 Summary analysis ............................................................ 273 6.5.1 The number of investigations within SVF increases .................... 274 6.5.2 Investigation within SVF should be based on medical assessment ....................................... 275.5.5.3 Primary care sees advantages with Svf, but complies with a symptoms, but a symptom a symptom, but complies with svf Various waiting times contribute to the system being perceived as complex ............ 278 6.5.5 The proportion of patients with SVF who receive a cancer diagnosis is uncertain .................................... 279 6.5.6 Expressing effects from SVF are highlighted, but Documentation is missing ............................... 280 6.5.7 70 6.5.7.7 280 6.5.7 ............................................ 281 6.5.8 Lack of data quality despite extensive administration ...........................
PowerPoint演示 div>
• Use cream containing urea or salicylic acid to soften hyperkeratotic areas areas • Clobetasol o betamethasone can help in symptom relief and treatment for lesions • Topical lidocaine can help in pain control • Cooling hand and foot baths containing magnesium sulphate can reduce pain • Oral analgesic in some cases • Refer patient to dermatologist in special cases
祝贺Achri的Morris Scantlebury博士成为Anthony N. Sabga Awards,Caribbean Excellenc
Neuroticism and extraversion as predictors of first-lifetime onsets of depression, anxiety, and suicidality in high-risk adolescents , Dr. Daniel Kopala-Sibley Association of epidural analgesia in labor with neurodevelopmental outcomes in premature infants born at <29 weeks of gestational age , Dr. Abhay Lodha Impact of Cytochrome P450 Genetic Variation on Patient-Reported Symptom氟西汀治疗的儿童和青少年的改善和副作用,DR。Paul Arnold&Chad BousmanPaul Arnold&Chad Bousman
有针对性的免疫调节剂用于治疗中等...
AAD American Academy of Dermatology AE Adverse Event BI Budget impact BSA Body Surface Area CMS Centers for Medicare and Medicaid Services CUA Cost utility analysis DC Discontinuation DIC Deviance information criterion DLQI Dermatology Life Quality Index dPGA Dynamic Physician Global Assessment EADV European Association for Dermatology and Venereology ERG Evidence Review Group EQ-5D EuroQol five-dimension questionnaire GDP Gross domestic product HRQL Health-related quality of life ICER Incremental cost-effectiveness ratio IGA Investigator's Global Assessment IPC International Psoriasis Council LY Life year MACE Major adverse cardiac events MCS Mental component score NHE National Health Expenditures NICE National Institute for Health and Care Excellence NMA Network meta-analysis NMSC Non-melanoma skin cancer PASI Psoriasis Area and Severity Index PCS Physical component score PDI Psoriasis Disability Index PGA Physician Global Assessment PRISMA Preferred Reporting Items for Systematic Reviews and Meta-Analyses PSD Psoriasis Symptom Diary PSI Psoriasis Symptom Inventory PSOLAR Psoriasis Longitudinal Assessment and Registry PUVA Psoralen and ultraviolet A radiation QALY Quality-adjusted life year RCT Randomized controlled trial Resdev Residual deviance SF-36短表36 SPGA静态医师全球评估TB结核病TNF肿瘤坏死因子USPSTF美国预防服务工作组UVB Ultraviolet B VAS VAS视觉模拟量表WAC批发批量审查成本成本wlq工作限制WPAI WPAI WPAI WPAI WPAI WORKITITION和ACTIVIC

Avey:一种用于自我诊断的精确 AI 算法
医疗自我诊断算法(或症状检查器)正日益成为数字健康和我们日常生活中不可或缺的一部分。在本文中,我们介绍了基于人工智能 (AI) 的症状检查器 Avey。同时,我们提出了一种全面的实验方法,利用标准临床插图方法来评估症状检查器。基于此方法,我们编制并同行评审了迄今为止该领域最大的基准插图套件。之后,我们定义了七个准确度指标,并利用这个插图套件从不同角度评估 Avey 和其他五种流行症状检查器的性能。此外,我们将 Avey 的准确度与三名平均经验为 16.6 年的经验丰富的初级保健医生进行了比较。结果显示,Avey 的表现明显优于五种症状检查器,并且比医生的表现更佳。

人工智能在医疗保健中的症状检查 人工智能的定义是“能够执行通常需要人类智能的任务的计算机系统的理论和开发,例如视觉感知、语音识别、决策和语言之间的翻译。”
人工智能在医疗保健中的症状检查 人工智能的定义是“能够执行通常需要人类智能的任务的计算机系统的理论和开发,例如视觉感知、语音识别、决策和语言之间的翻译。”

Avey:一种用于自我诊断的精确人工智能算法
目标 介绍我们基于人工智能的症状检查器,严格测量其准确性,并将其与现有的流行症状检查器和经验丰富的初级保健医生进行比较。 设计案例研究。 设置 400 个黄金标准初级保健案例。 干预/比较器我们使用了 7 个标准准确性指标来评估 6 个症状检查器的性能。为此,我们开发并同行评审了 400 个案例,每个案例都得到了 7 名独立且经验丰富的全科医生中至少 5 名的认可。据我们所知,这产生了迄今为止该领域最大的基准案例套件。 为了建立参考框架并相应地解释症状检查器的结果,我们进一步将表现最佳的症状检查器与 3 名平均经验为 16.6 年的初级保健医生直接进行比较。主要结果测量我们从 7 个标准角度彻底研究了症状检查者和医生的诊断准确率,包括:(a) 𝑀 1、𝑀 3 和 𝑀 5 分别作为症状检查者或医生在前 3 种疾病中或前 5 种鉴别诊断疾病中返回小插图主要诊断的能力的测量指标;(b) 召回率作为症状检查者或医生鉴别诊断中返回的相关疾病百分比的测量指标;(c) 精确度作为症状检查者或医生鉴别诊断中相关疾病百分比的测量指标;(d) F1 测量作为召回率和精确度之间的权衡测量指标;(e) 归一化折现累积增益或 NDCG 作为症状检查者或医生鉴别诊断排名质量的测量指标诊断。结果 我们的基于 AI 的症状检查器 Avey 的表现明显优于 5 种流行的症状检查器,即 Ada、WebMD、K Health、Buoy 和 Babylon,使用 𝑀 1 时平均高出 24.5%、175.5%、142.8%、159.6%、2968.1%;使用 𝑀 3 时平均高出 22.4%、114.5%、123.8%、118.2%、3392%;使用 𝑀 5 时平均高出 18.1%、79.2%、116.8%、125%、3114.2%;使用召回率时平均高出 25.2%、65.6%、109.4%、154%、3545%;使用 F1 测量时分别为 8.7%、88.9%、66.4%、88.9%、2084%;使用 NDCG 时分别为 21.2%、93.4%、113.3%、136.4%、3091.6%。在精度方面,Ada 平均比 Avey 高出 0.9%,而 Avey 分别比 WebMD、K Health、Buoy 和 Babylon 高出 103.2%、40.9%、49.6% 和 1148.5%。与症状检查员相反,医生在使用精确度和 F1 测量时比 Avey 平均高出 37.1% 和 1.2%,而 Avey 在使用 𝑀 1、𝑀 3、𝑀 5、召回率和 NDCG 时分别比他们平均高出 10.2%、20.4%、23.4%、56.4% 和 25.1%。为了提高我们研究的可重复性并支持未来的相关研究,我们公开并免费提供了所有黄金标准小插图。此外,我们在网上发布了症状检查员和医生的所有结果(即 45 组
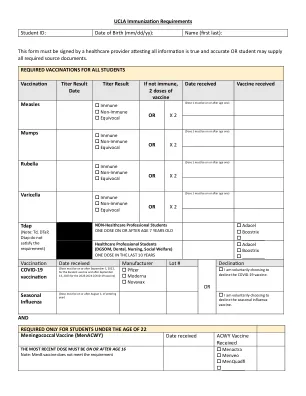
出生日期(mm/dd/yy):名称(第一个最后):此表格必须...
TUBERCULOSIS SYMPTOM REVIEW – Check all appropriate boxes Cough lasƟng more than 3 weeks: No Yes Excessive sputum: No Yes Coughing up blood: No Yes Excessive faƟgue/malaise: No Yes Unexplained/unintended weight loss (> 5lbs): No Yes Recent unprotected close contact with a person with acƟve TB: No Yes Night sweats (not related to menopause): No Yes History of immune dysfuncƟon or are you receiving chemotherapeuƟc or immunosuppressant agents: No Yes Fever/chills: No Yes Allergies: No known Allergies Yes: *If you have any of the above symptoms, meet with your provider to determine whether a chest x-ray is indicated.

itovebi(inavolisib)片剂,用于口服-AccessData.fda.gov
itovebi+p+f =带有palbociclib和fulvestrant臂的itovebi;安慰剂+p+f =安慰剂,带有palbociclib和fulvestrant臂。a症状属性评分是由数量/频率/严重性定义的,得分为0 ='完全不'/'nover'/''/none'; 1 ='稍加'/'少一点'/'温和'; 2 =“有点”/“偶尔”/“中等”; 3 =“有点”/“经常”/“严重”; 4 =“非常”/“几乎不断”/“非常严重”。b治疗前症状评分的患者百分比为1-4。 C在治疗前的分数方面,症状评分增加的患者百分比。d在治疗前的分数方面,症状评分在治疗期间的患者百分比增加到3或4。e在治疗前提供评分和至少一个在治疗评分之前的患者人数。
