机构名称:
¥ 1.0
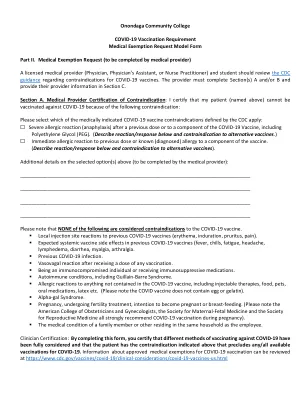
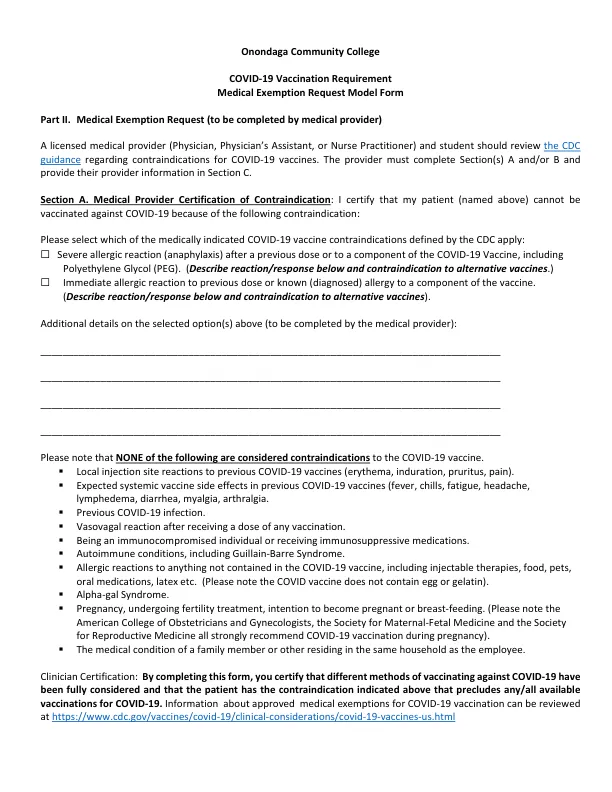
Onondaga社区学院COVID -199疫苗接种要求医疗豁免请求模型第二部分。医疗豁免请求(由医疗提供者完成)持牌医疗提供者(医师,医师的助理或护士从业者),学生应审查有关COVID -19疫苗禁忌症的CDC指南。提供商必须填写第A和/或B节,并在C节中提供其提供者信息。Medical Provider Certification of Contraindication : I certify that my patient (named above) cannot be vaccinated against COVID‐19 because of the following contraindication: Please select which of the medically indicated COVID‐19 vaccine contraindications defined by the CDC apply: ☐ Severe allergic reaction (anaphylaxis) after a previous dose or to a component of the COVID‐19 Vaccine, including Polyethylene糖(钉)。(描述下面的反应/反应,以及对替代疫苗的禁忌症。)☐对先前剂量或已知(诊断)过敏的直接过敏反应对疫苗的成分。(描述下面的反应/反应以及替代疫苗的禁忌症)。Additional details on the selected option(s) above (to be completed by the medical provider): ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ Please note that NONE of以下被认为是共vid -19疫苗的禁忌症。
COVID-19-19S医学豁免表第二部分。 ...COVID-19-19S医学豁免表第二部分。 ...
主要关键词
相关文件推荐