机构名称:
¥ 1.0
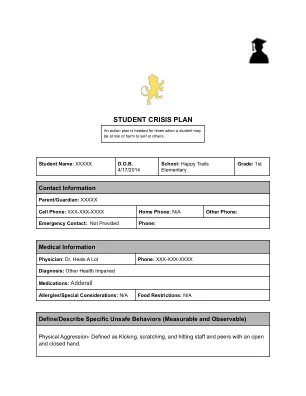
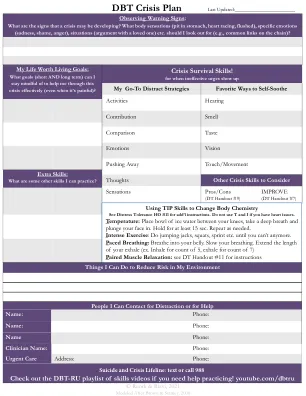
当我感觉良好时,我的样子。迹象表明我需要支持者,如果我有以下几个迹象和/或症状,请致电下一页命名的支持者。Information on Medications / Supplements / Health Care Information Physician ______________________ Psychiatrist ________________________ Other Health Care Providers: Pharmacy ______________________ Pharmacist ______________________________ Allergies Insurance Information ____________________________________________________ Medication / Supplement / Health Care Preparation I am currently using Dosage ___________________________Purpose________________________ Medication / Supplement / Health Care Preparation I am currently using Dosage ___________________________Purpose Treatments and Complementary Therapies that work well for me Treatment/Complementary Therapy _______________________________________________________________________ When and how to use this treatment/complementary therapy _______________________________________________________________________
个人危机计划
主要关键词
相关文件推荐