机构名称:
¥ 1.0
一般信息您是向我们的办公室转介吗?是,如果是,我们可以感谢谁转介?_________________________ Phone: _____________ Address: __________________________________________________________________________ Child's Full Name: __________________________________________________ Male/ Female Birth Date: _________________________ Age: _____ years ______ months Name of School: __________________________________________ Grade: ________ Teacher: _______________________校长:________________________________您的孩子特别害怕医生吗?_________________________________________ Child's dominant hand (circle): right or left ?是否有使用手的指导?Yes No Father's Name: _________________________ Mother's Name:______________________________ Daytime Phone:__________________________ Evening Phone:_______________________________ Cell Number:_____________________________________ Email Address:____________________________________________________________
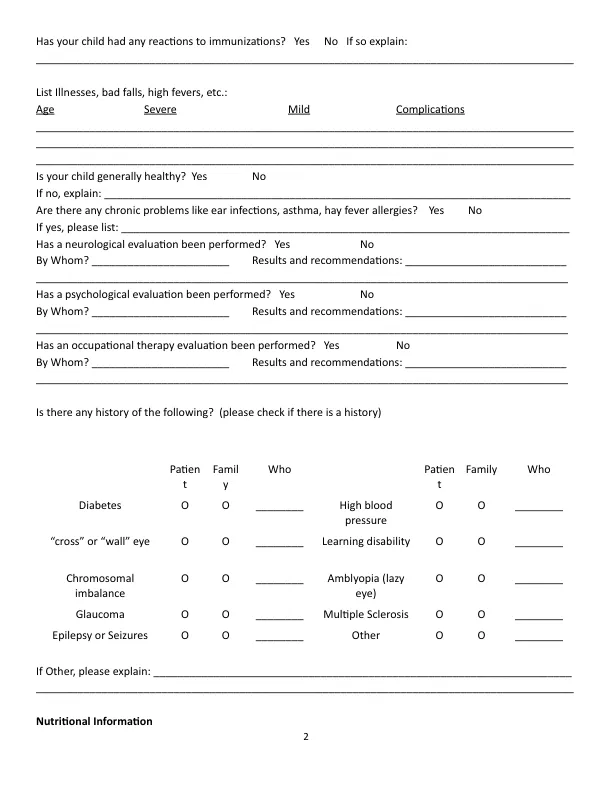
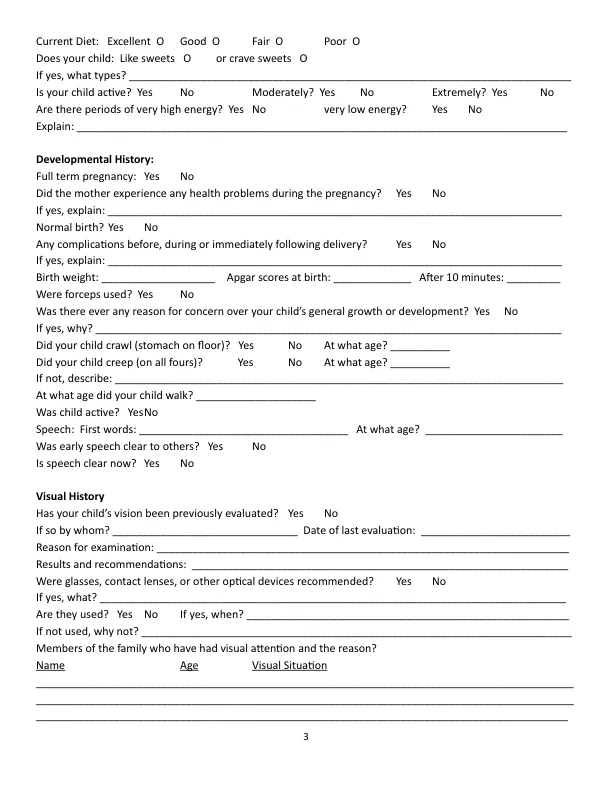
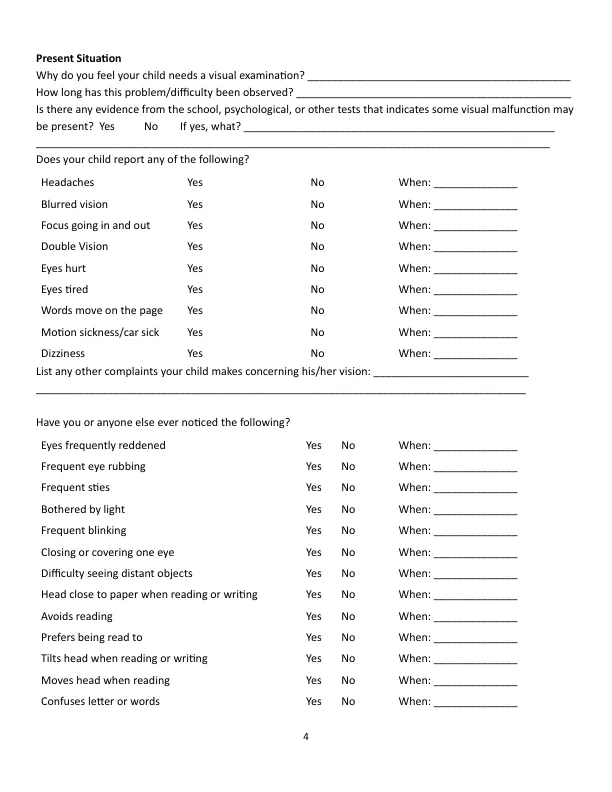
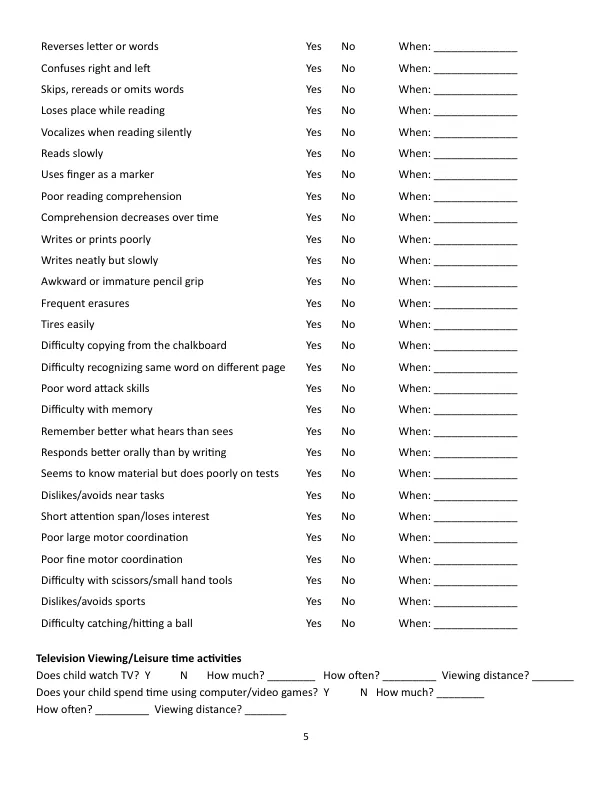
儿童视力问卷
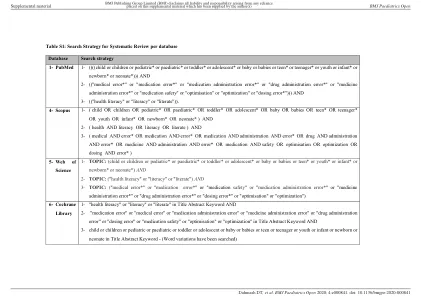
主要关键词
相关文件推荐