机构名称:
¥ 1.0
Supervisor's Comment Period of Supervision from _____________till _______ ____ I certify that the above candidate has fulfilled his/her training and practicing hours to apply for the *certification/re-certification Diabetes Educator program.签名:日期:主管的姓名和指定 *相应删除
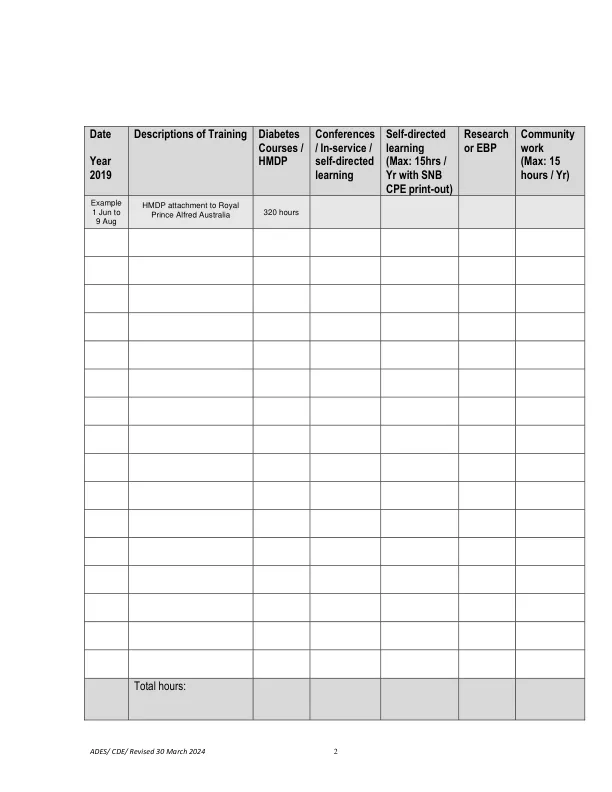
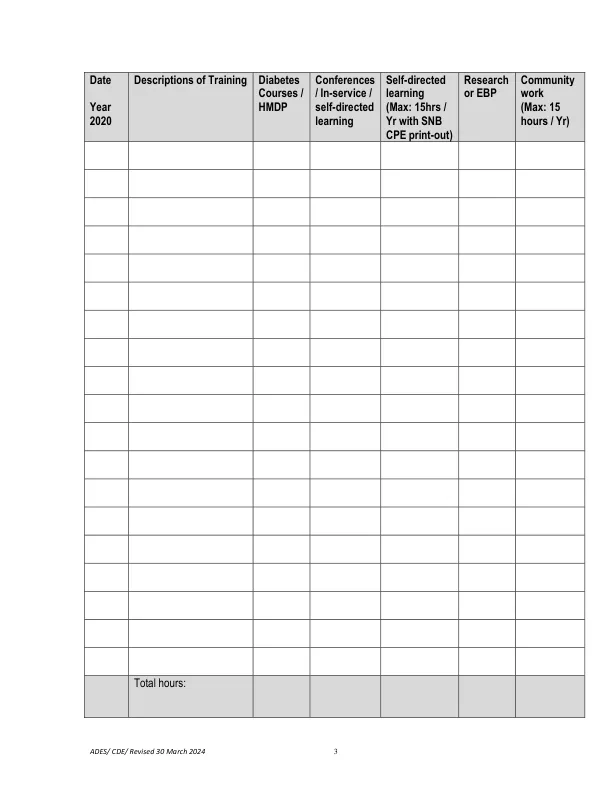
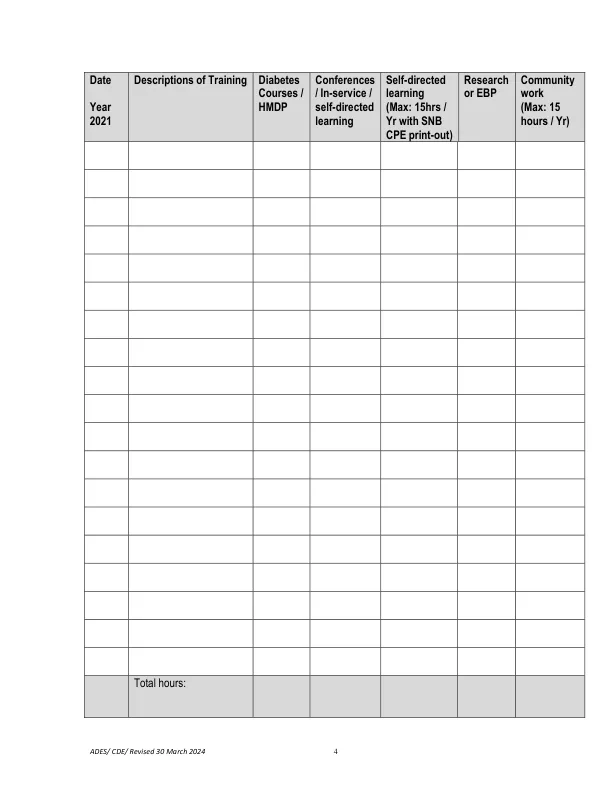
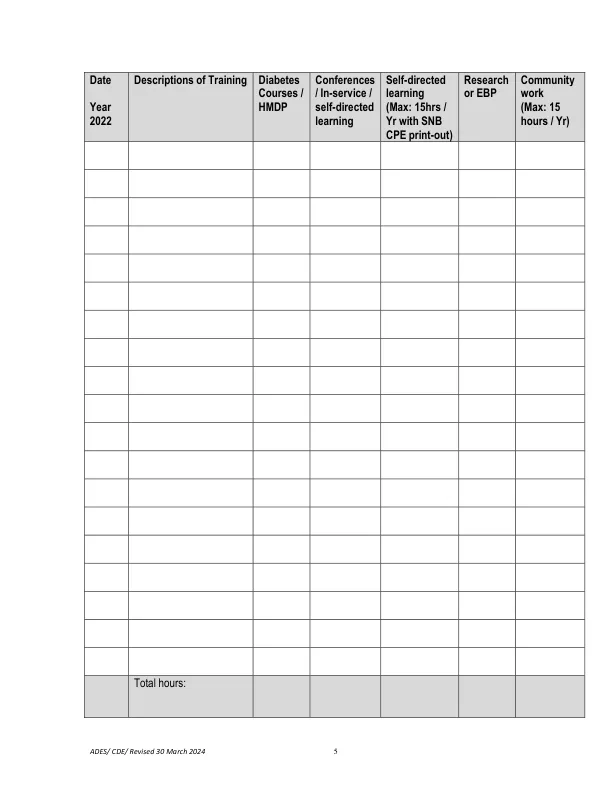
糖尿病教育者的培训日志 - ADES
主要关键词
相关文件推荐