机构名称:
¥ 1.0
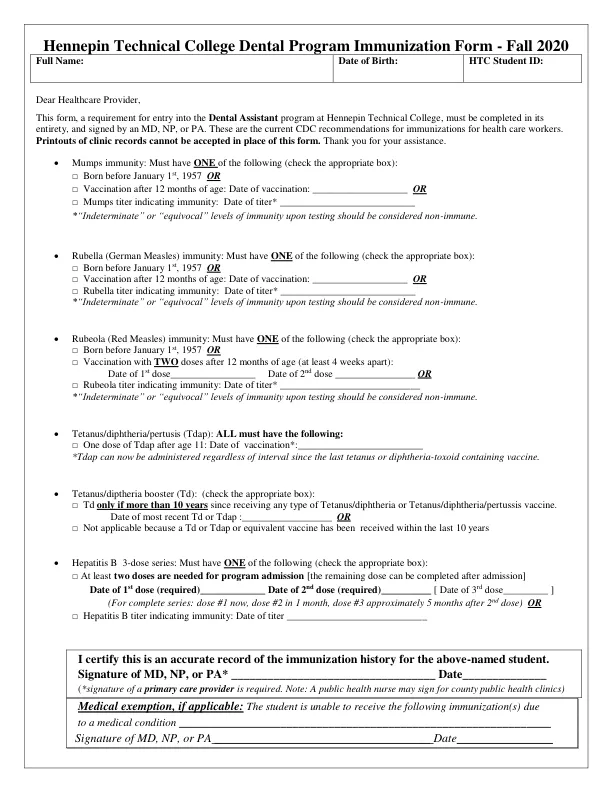
Mumps immunity: Must have ONE of the following (check the appropriate box): □ Born before January 1 st , 1957 OR □ Vaccination after 12 months of age: Date of vaccination: ___________________ OR □ Mumps titer indicating immunity: Date of titer* ___________________________ *“Indeterminate” or “equivocal” levels of immunity upon testing should be considered非免疫。 Rubella (German Measles) immunity: Must have ONE of the following (check the appropriate box): □ Born before January 1 st , 1957 OR □ Vaccination after 12 months of age: Date of vaccination: ___________________ OR □ Rubella titer indicating immunity: Date of titer* ___________________________ *“Indeterminate” or “equivocal” levels of immunity upon testing should be considered非免疫。 Rubeola (Red Measles) immunity: Must have ONE of the following (check the appropriate box): □ Born before January 1 st , 1957 OR □ Vaccination with TWO doses after 12 months of age (at least 4 weeks apart): Date of 1 st dose_________________ Date of 2 nd dose ________________ OR □ Rubeola titer indicating immunity: Date of titer* ____________________________ *测试时的“不确定”或“模棱两可”的免疫力应视为非免疫性。破伤风/白喉/域(tdap):所有人必须具有以下内容:□11岁以后的一剂TDAP:疫苗接种日期 *:_________________________________ *现在,无论是自上次的tetanus或diphtheria contania coctine以来,都可以给予TDAP。破伤风/白皮亚助推器(TD):(选中适当的框):□TD仅当收到任何类型的破伤风/白喉或破伤风/破伤风/二甲状腺/diphtheria/disttussis疫苗以来,只有10年以上。Date of most recent Td or Tdap :__________________ OR □ Not applicable because a Td or Tdap or equivalent vaccine has been received within the last 10 years Hepatitis B 3-dose series: Must have ONE of the following (check the appropriate box): □ At least two doses are needed for program admission [the remaining dose can be completed after admission] Date of 1 st dose (required)_____________ Date of 2 nd dose (required)__________ [ Date of 3 rd dose_________ ] (For complete series: dose #1 now, dose #2 in 1 month, dose #3 approximately 5 months after 2 nd dose) OR □ Hepatitis B titer indicating immunity: Date of titer ____________________________ I certify this is an accurate record of the immunization history for the above-named student.Signature of MD, NP, or PA* __________________________________ Date______________ ( *signature of a primary care provider is required.Note: A public health nurse may sign for county public health clinics) Medical exemption, if applicable: The student is unable to receive the following immunization(s) due to a medical condition ______________________________________________________________ Signature of MD, NP, or PA ____________________________________ Date________________
牙科免疫 - pdf
主要关键词
相关文件推荐