机构名称:
¥ 1.0
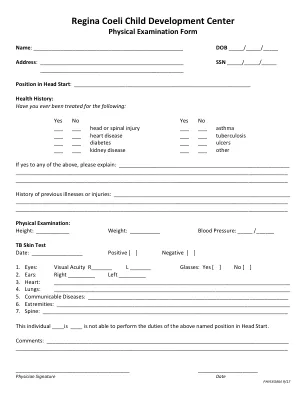
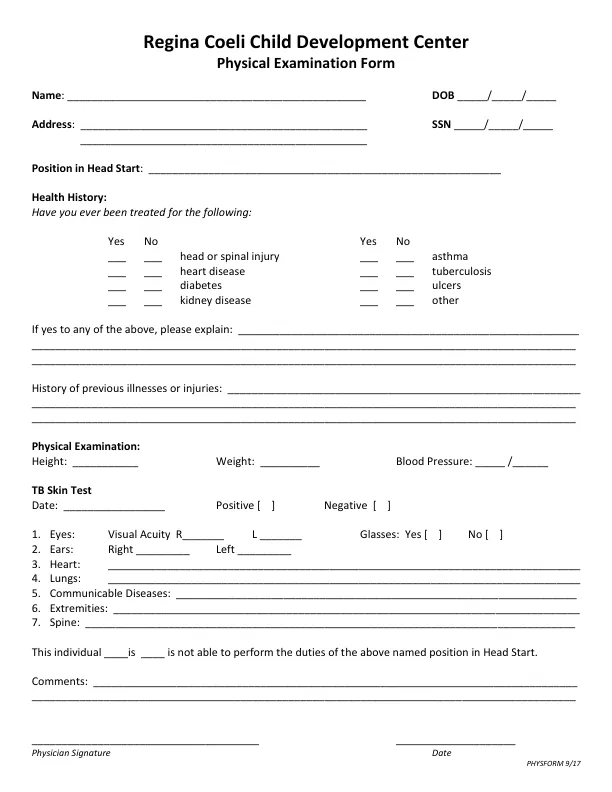
Yes No Yes No ___ ___ head or spinal injury ___ ___ asthma ___ ___ heart disease ___ ___ tuberculosis ___ ___ diabetes ___ ___ ulcers ___ ___ kidney disease ___ ___ other If yes to any of the above, please explain: _________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ History of previous illnesses or injuries: ___________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ Physical Examination: Height: ___________ Weight: __________ Blood Pressure: _____ /______ TB Skin Test Date: _________________ Positive [ ] Negative [ ] 1.眼睛:视力r______ l _______眼镜:是[]否[] 2。耳朵:右_________左_________ 3。心:__________________________________________________________________________________________________________________________________________________________________________________一些 肺:_________________________________________________________________________________________________________________________________________________________________________________________________________________多 传播疾病:___________________________________________________________________________ 6。 四肢:_____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________一些。 Spine: __________________________________________________________________________________ This individual ____is ____ is not able to perform the duties of the above named position in Head Start.心:__________________________________________________________________________________________________________________________________________________________________________________一些肺:_________________________________________________________________________________________________________________________________________________________________________________________________________________多传播疾病:___________________________________________________________________________ 6。四肢:_____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________一些。Spine: __________________________________________________________________________________ This individual ____is ____ is not able to perform the duties of the above named position in Head Start.Comments: _________________________________________________________________________________ ___________________________________________________________________________________________ ______________________________________ ____________________ Physician Signature Date
Regina Coeli儿童发展中心
主要关键词
相关文件推荐