机构名称:
¥ 1.0
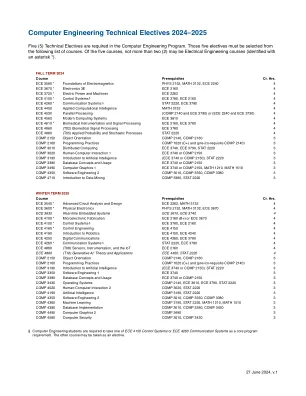
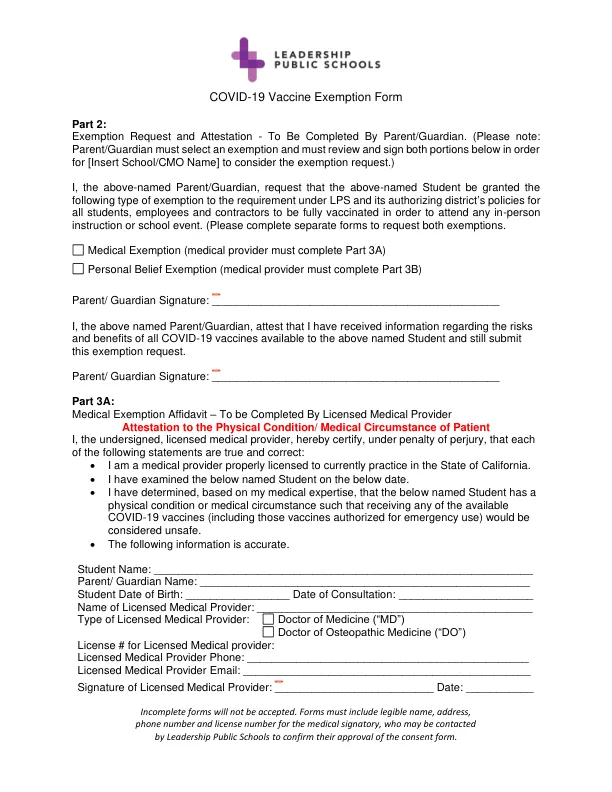
•我是一名医疗提供者,并获得了当前在加利福尼亚州执业的许可。•我在以下日期检查了以下名称的学生。•我根据我的医学专业知识确定了以下名称的学生具有身体状况或医疗状况,因此接收任何可用的Covid-19疫苗(包括授权紧急使用的疫苗)将被视为不安全。•以下信息是准确的。Student Name: ______________________________________________________________ Parent/ Guardian Name: ______________________________________________________ Student Date of Birth: _________________ Date of Consultation: ______________________ Name of Licensed Medical Provider: _____________________________________________ Type of Licensed Medical Provider: Doctor of Medicine (“MD”) Doctor of Osteopathic Medicine (“做”)许可医疗提供者的许可证#:许可医疗提供者电话:___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
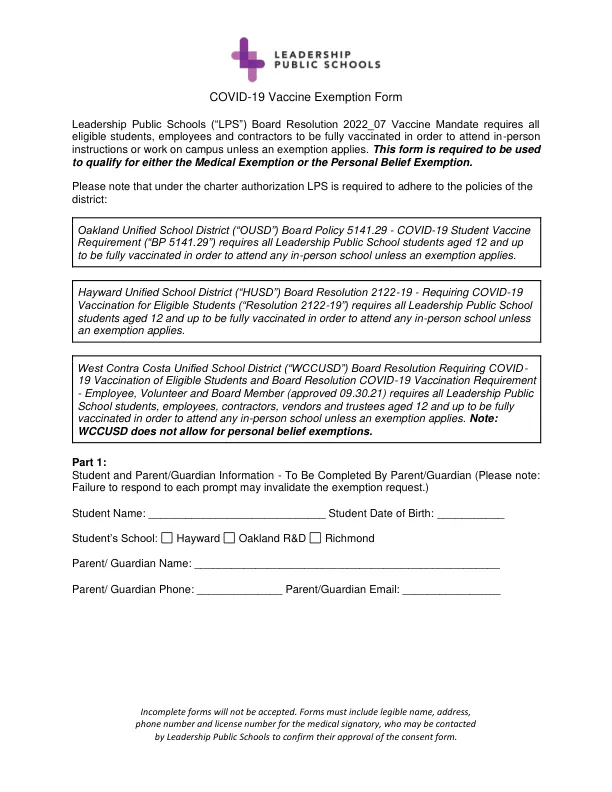
covid-19疫苗豁免表
主要关键词

相关文件推荐