机构名称:
¥ 1.0
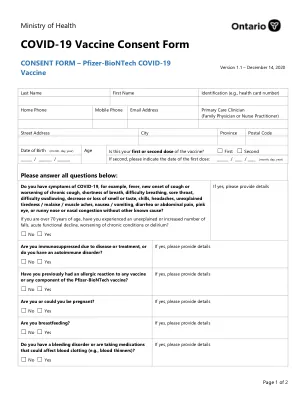
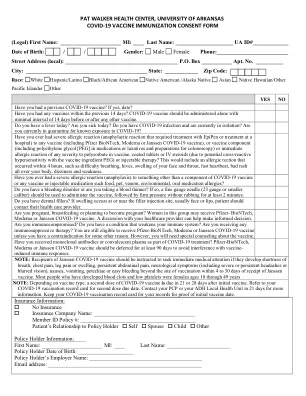
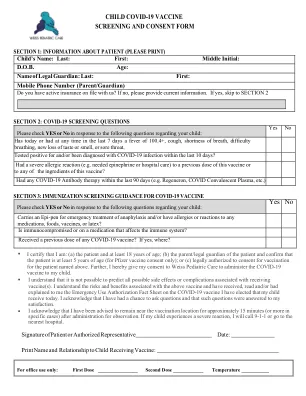
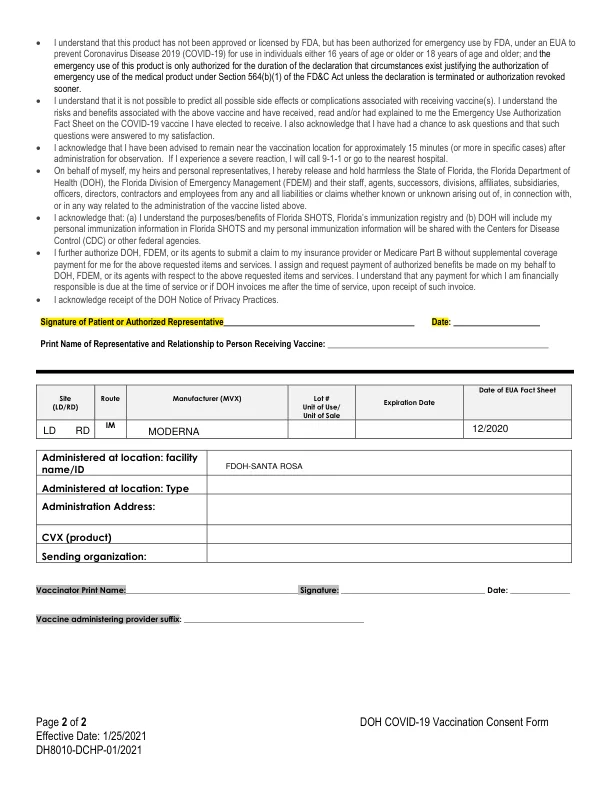
Ethnicity ☐ Hispanic or Latino ☐ Not Hispanic or Latino ☐ Unknown Primary Insurance Carrier ID #: ______________________Grp #: ____________________ Insurance Company : ____________________________________________Insurance Company Phone #_____________________ Insured's Name:________________________________Relationship:_______________________Insured's Date of Birth___________ Secondary Insurance Carrier ID #: ______________________Grp #: ____________________ Insurance Company : ____________________________________________Insurance Company Phone #_____________________ Insured's Name:________________________________Relationship:_______________________Insured's Date of Birth___________ Is this the patient's first or second dose of the COVID-19 vaccination?☐第一次剂量☐第二剂量第2节:covid-199筛选问题
covid-19疫苗筛查和同意形式
主要关键词

相关文件推荐