
机构名称:
¥ 1.0
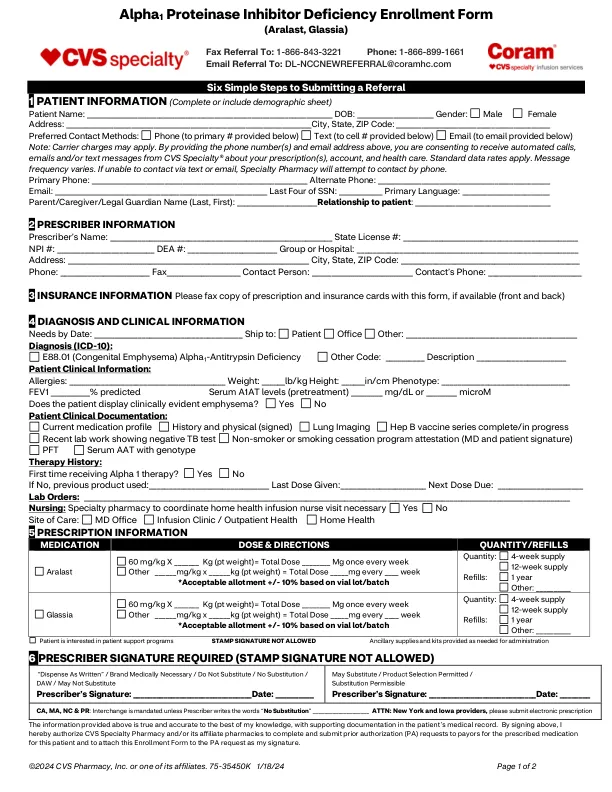
Six Simple Steps to Submitting a Referral 1 PATIENT INFORMATION (Complete or include demographic sheet) Patient Name: ___________________________________________________________________ DOB: _____________________ Gender: Male Female Address: ___________________________________________________________________City, State, ZIP Code: __________________________________________ Preferred Contact Methods: Phone (to primary # provided below) Text (到下面提供的单元格#)电子邮件(下面提供的电子邮件)注意:运营商费用可能适用。通过提供上面的电话号码和电子邮件地址,您同意从CVSSpecialty®收到有关您的处方,帐户和医疗保健的自动电话,电子邮件和/或短信。适用标准数据速率。消息频率各不相同。如果无法通过文本或电子邮件联系,专业药房将尝试通过电话联系。Primary Phone: ___________________________________________________________ Alternate Phone: _______________________________________________ Email: __________________________________________________________ Last Four of SSN: ____________ Primary Language: ________________________ Parent/Caregiver/Legal Guardian Name (Last, First): ______________________ Relationship to patient : _____________________________________
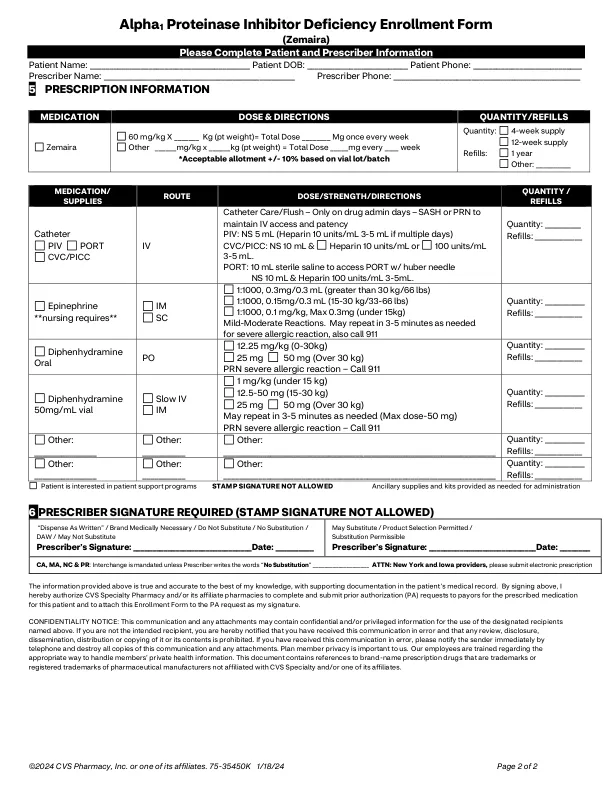
alpha1蛋白酶抑制剂缺乏症形式
主要关键词
相关文件推荐







![Prolastin®-C(Alpha1-蛋白酶抑制剂[人])](/simg/7/7cb6fccce4845c28297f180a577afcab5d471cab.webp)












![Prolastin®-C 液体(Alpha1-蛋白酶抑制剂 [人])](/simg/6/6d9e015c830469fbfd459a26956e8de3edd47546.webp)