机构名称:
¥ 1.0
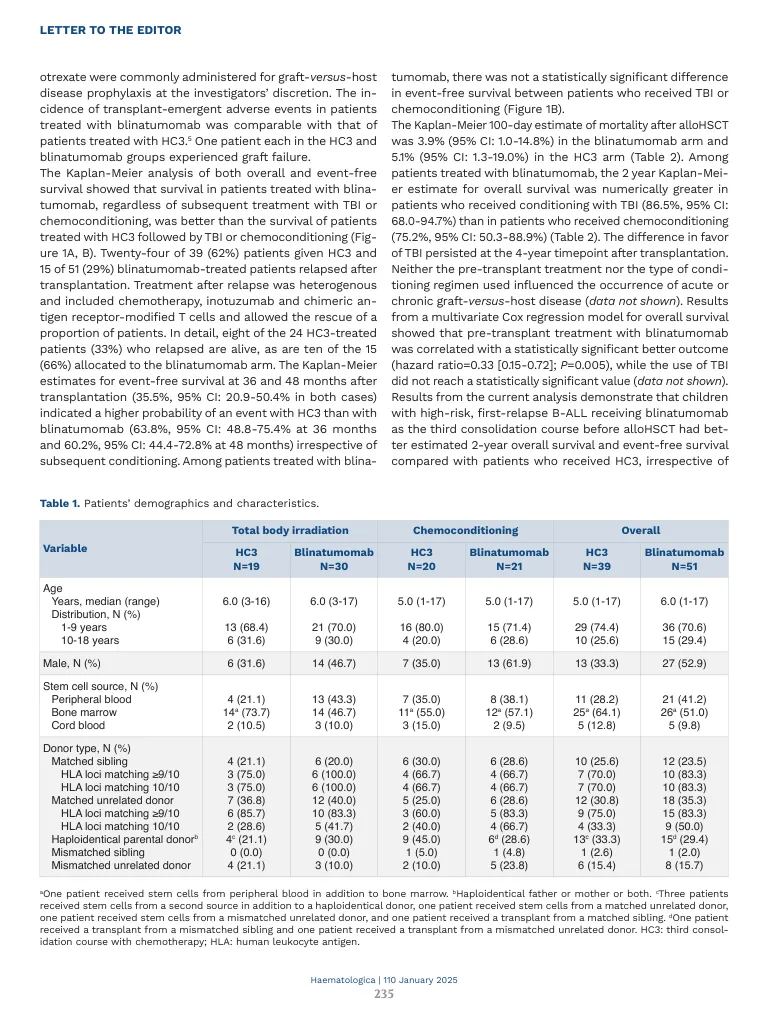
全身照射(TBI)是在同种异体血液诗歌干细胞移植(ALLOHSCT)之前给予许多结合治疗方案的关键组成部分,急性淋巴细胞性白血病患者(全部)。最近的一项大型随机临床研究 - 包括≥9/10 HLA基因座的患者,表明患有高风险/复发的儿童所有接受TBI PLUS ETOPOSIDE作为调理方案的儿童具有明显更高(P <0.0001)2年生存率(0.91),95%Cifival Intervial Intervials [95%CI]。在进行AlloHSCT之前,他会采用化学疗法(化学解决方案; 0.75,95%CI:0.67-0.81)进行调节。1虽然有效,但使用TBI的调理与终身不良反应的风险有关,包括生长损害,性腺,甲状腺和认知功能,白内障的发生率增加和继发性恶性肿瘤。2-4因此,旨在提供基于TBI的条件的替代方案的新方法是理想的。blinatumomab是一种双特异性T细胞参与者,它将CD3阳性T细胞重定向以接合和裂解CD19阳性靶细胞。一项随机的,III期试验(NCT02393859)的恶魔,与一个blinatumomab的一个周期相比,与标准的强化多重多药化疗相比,该治疗是在小儿高危B-cell(b-cell a aillohsct)之前作为第三个巩固疗程(HC3)进行的。研究设计的细节,患者的资格以及blinatumomob和hc3的治疗剂量已在其他地方报道。5,6 In order to better dissect the contri bution of immediate pre-transplant treatment from the role played by the conditioning regimen, we performed a post hoc analysis aimed at evaluating the outcome of children with high-risk, first-relapse B-ALL from this phase III study who received either blinatumomab or chemotherapy (HC3) as the third consolidation course and for whom data on the type of conditioning regimen received (TBI或化学处理)在AllOHSCT之前可用。5高风险的首次复发已经定义。7,8例在用Blinatumomab或HC3治疗后获得或维持第二次完全缓解的患者被分配在AlloHSCT前接受TBI或化学调节。在AlloHSCT进行之前的骨髓性调节(6个馏分中为12 Gy)加60 mg/kg依托泊苷(1.8 g/m 2;总剂量3.6 g)或包括氟达滨(氟达滨)(每天30 mg/m 2)的最大总剂量3.6 g)
blinatumomab与更好的后移植
主要关键词



相关文件推荐