机构名称:
¥ 1.0
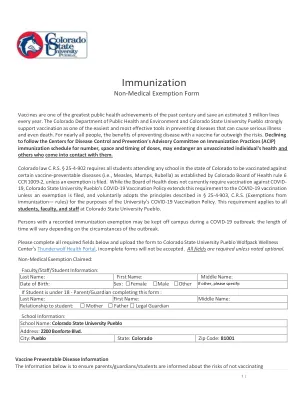
__________ I understand that I may be required to adhere to disease control strategies recommended by public health authorities for non-vaccinated individuals, including but not limited to wearing a mask, practicing social distancing, being isolated/quarantined from campus, and/or being excluded from campus and/or college activities (e.g., classes, activities, travel, and on-campus housing) for the protection of my personal health and the health of the community, as determined by Mount霍利奥克学院和/或地方,州或联邦公共卫生当局。__________我知道我的豁免请求将逐案评估,不是自动的,如果不合理的话,可能不会被授予,对我本人或他人的健康和安全构成直接威胁,或者对霍利奥克山学院造成了不当的艰辛。Student signature: ____________________________________________________________________________ Date: __________________________ If student is under 18, a parent or guardian must also sign: Print Name:__________________________________________________________________________________ Relation:_________________________ Signature:______________________________________________________________________________________ Date: __________________________
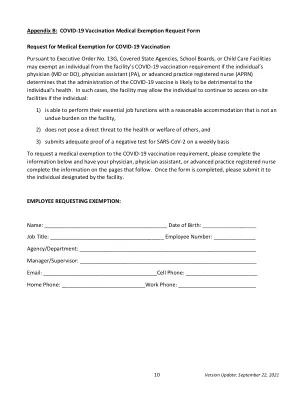
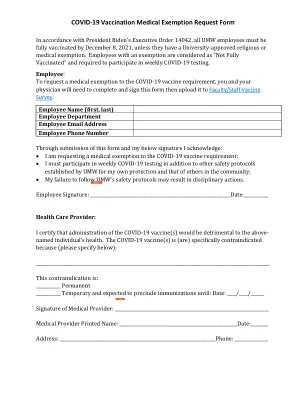
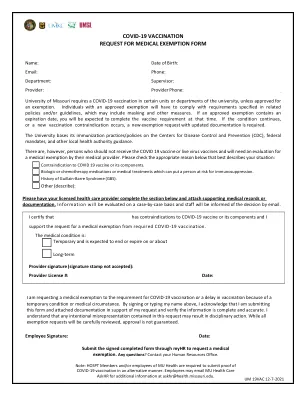
医疗疫苗豁免请求表
主要关键词
相关文件推荐